A group led by researchers from Kobe University has illuminated clinical factors that are related to the occurrence of congenital cytomegalovirus (CMV) infection in newborns. They revealed for the first time in the world that fever or cold-like symptoms (including cough, sore throat and runny nose) during pregnancy, and threatened miscarriage or threatened premature labor (*1) in the second trimester (14-27 gestational weeks) were associated with CMV infection in newborns.
The cross-institutional research group consisted of Kobe University Graduate School of Medicine’s Professor YAMADA Hideto (Department of Obstetrics and Gynecology), Nihon University School of Medicine’s Professor MORIOKA Ichiro (Department of Pediatrics and Child Health) and Director MINEMATSU Toshio (of Aisenkai Nichinan Hospital’s Research Center for Disease Control), among others.
Recent research conducted by this team and others has indicated that the blood tests currently carried out on pregnant women might not be effective in determining the likelihood of congenital CMV infection in newborns. This research has illuminated clinical factors during pregnancy that could be used to predict the occurrence of congenital CMV infection without relying on blood tests. This would allow at-risk newborns to be comprehensively tested and treated immediately when necessary; hopefully reducing the number of children suffering from the aftereffects of congenital CMV infection.
The results of this research were published in the American scientific journal ‘Clinical Infectious Diseases’ on January 14, 2020.
Main points
- Cytomegalovirus can infect fetuses, causing mental and physical development issues as well as hearing difficulties in newborns.
- Recently, it has been reported that early treatment with antiviral drugs can ameliorate loss of hearing and delayed mental development. Therefore, the early detection of newborns with congenital CMV infection is highly important.
- As it was previously thought that the majority of CMV infected newborns were born to mothers who were initially infected during the pregnancy, maternal blood tests (for example, serology tests that detect antibodies) have been used to screen (*2) for the virus. However, there are in fact more newborns with congenital CMV infection whose mothers had the virus prior to the pregnancy as opposed to mothers who contracted the virus during the pregnancy. The severe aftereffects in newborns remain the same in both cases. Serology tests may be unable to predict the occurrence of congenital CMV infection in mothers who were infected prior to the current pregnancy.
- The research team looked for clinical factors during pregnancy that could be used to predict congenital CMV infection occurrence without relying on blood tests.
Research Background
Research has focused on CMV because it can cause severe aftereffects if it infects the fetus, including issues with mental and physical development and hearing loss. It is a big issue worldwide; for example, it is estimated that around 1000 babies are born with congenital CMV infections every year in Japan.
Presently there are no effective vaccines or treatments available, therefore screening all pregnant women for CMV has been discouraged. However, it has recently been revealed that prompt treatment of affected newborns with antiviral drugs can improve mental and hearing outcomes. Consequently, the importance of accurate detection of congenital CMV infections in infants prior to birth has been reasserted.
Until recently, it was thought that newborns with congenital CMV infection were born to mothers who initially acquired the infection during pregnancy (primary infection). For this reason, maternal serological screening, such as blood tests for CMV-specific immunoglobin (Ig) M (*3), IgG antibodies (*4), and CMV IgG avidity tests(*5), were considered effective for detecting pregnancies with a high risk of congenital CMV infection.
However in recent years, many researchers from around the world reported that there were more infected babies born to pregnant women with chronic CMV infection prior to the affected pregnancy than those born to pregnant women with primary CMV infection. In addition, the severity of the symptoms in newborns was similar regardless of when the mother was infected. This research group also published results indicating this in ‘Clinical Infectious Diseases’ in 2017. These research studies illuminated the dangers of congenital CMV infection being overlooked in some cases due to the ineffectiveness of serological screening.
Ideally, universal screening for CMV-DNA in urine samples of newborns using PCR (*6) would be able to detect all cases of congenital CMV infection, however there are currently no countries that carry out CMV PCR on all newborns. As universal neonatal screening is not practical, it would be more realistic to detect babies at high risk of congenital CMV infection prior to birth and subsequently test their urine after birth.
This research study on pregnant women who gave birth at a primary maternity hospital sought to determine whether there were any clinical factors during pregnancy that were predictive of congenital CMV infection occurrence, without using serological screening.
Research Methodology
The cohort study was carried out on 4,125 low-risk pregnant women who received consultation and gave birth at Nadeshiko Ladies Hospital (a primary maternity hospital affiliated with Kobe University) between March 2009 and November 2019.
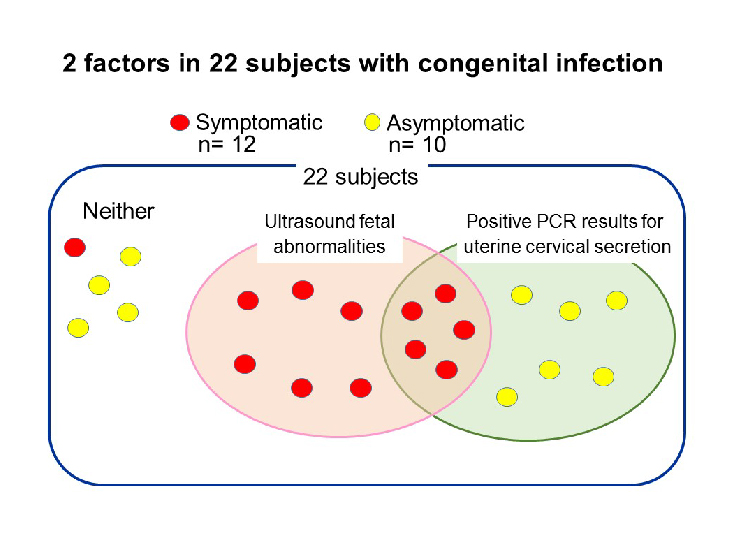
CMV PCR tests were conducted using urine samples from all of the infants born during the research period, nine (0.2%) of which had congenital CMV infection. Among these nine, one newborn had hearing problems. In order to determine the factors that increase the likelihood of congenital CMV infection occurrence, the research group collected the following clinical data on the all pregnant women in the study:
- Age
- Gravity and parity
- BMI prior to pregnancy
- Occupation
- Smoking history
- Fertility treatment history
- Presence of fever or cold-like symptoms during pregnancy
- History of maternal and obstetric complications; including threatened miscarriages, threatened premature labor, hypertensive disorders and gestational diabetes.
- Non-reassuring fetal status (*7) during labor
- Whether delivery was performed by Caesarian section.
- Gestational age at delivery
In addition, data on the newborns, including birth weight, sex, and hearing test screening results, was also compiled.
The results from pregnancies affected by CMV and unaffected pregnancies were compared through statistical analysis of the aforementioned clinical factors. It was determined that the percentage of pregnant women who had a fever or cold-like symptoms during pregnancy was higher among those who gave birth to newborns with congenital CMV infection, compared with those who did not. In addition, threatened miscarriage or threatened premature labor in the second trimester was experienced in a higher percentage of congenital CMV infection cases. Furthermore, the research group statistically proved that these clinical factors were associated with congenital CMV infection in newborns using logistical regression analysis.
Subsequently, the optimal predictive factors for congenital CMV infection occurrence were estimated. The presence of fever or cold-like symptoms during pregnancy yielded a sensitivity (*8) of 78% and a specificity (*9) of 85%. Threatened miscarriage or threatened premature labor in the second trimester had a sensitivity of 78% and a specificity of 61%. Furthermore, if a combination of these two symptoms was experienced, then the sensitivity was 100% with a specificity of 53%.
Based on these results, it is recommended that CMV PCR tests are conducted on the newborn’s urine if the mother experiences any of the above identified factors during pregnancy.
Conclusion
Blood tests have enabled primary infections of CMV during pregnancy to be diagnosed, yet have been unable to predict congenital CMV infection occurrence in pregnant women with chronic infections. This has resulted in numerous cases of congenital CMV infection being overlooked.
This research study was carried out to see if the occurrence of congenital CMV infection could be linked to clinical factors during pregnancy, to allow the likelihood of infection to be predicted without conducting blood tests. The results revealed that fever or cold-like symptoms during pregnancy, and threated miscarriage or threatened premature labor in the second trimester were factors linked to congenital CMV infection.
If these symptoms are experienced during pregnancy, carrying out PCR tests for CMV in the newborn’s urine would allow congenital infection to be diagnosed and treated sooner. It is hoped that this would reduce the number of babies suffering from the effects of congenital CMV.
Glossary
- 1. Threatened miscarriage/threatened premature labor
- Symptoms including lower abdominal pain, uterine contraction, genital bleeding and shortening of the uterine cervical length. If these symptoms worsen, there is a danger that miscarriage (under 21 gestational weeks) or premature birth (under 36 gestational weeks) will result.
- 2. Screening
- Medical methodology whereby a group, including healthy people, is tested for a certain disease to identify those who are infected and the predictive indicators of infection.
- 3. CMV IgM antibodies
- CMV Immunoglobin M antibodies are produced 1-2 weeks after the initial CMV infection but disappear after 2-3 months. Therefore, a positive IgM test indicates that primary CMV infection occurred within the last 3 months. However, there are also cases where subjects test positive for IgM years after the initial infection.
- 4. CMV IgG antibodies
- IgG antibodies are produced after IgM antibodies in response to an antigen. Unlike IgM antibodies which disappear 2-3 months after the initial infection, IgG antibodies continue to be produced for the rest of one’s life. Primary CMV infection is diagnosed if the presence of CMV IgG antibodies changes from negative to positive. If CMV IgM antibody tests are negative and CMV IgG are positive, this indicates that there is a chronic infection.
- 5. CMV IgG avidity test
- Avidity testing is used to determine how long a person has had an infection by determining how strongly antibodies bind to the antigens. During the initial period of infection IgG antibodies show low avidity; they bind weakly to the CMV antigens. On the other hand, when the patient has a chronic CMV infection, their IgG antibodies demonstrate higher avidity. This avidity test is used as an auxiliary test to diagnose primary infections in cases where CMV IgM antibody tests are positive.
- 6. PCR testing
- A method of testing for the presence of a disease by amplifying small samples of DNA.
- 7. Non-reassuring fetal status
- When there is insufficient oxygen in the womb during labor.
- 8. Sensitivity
- In statistics, the proportion of correctly identified positives. For example, the percentage of people with the disease who are correctly identified as having it.
- 9. Specificity
- In statistics, the proportion of correctly identified negatives. For example, the percentage of healthy people who were correctly diagnosed as healthy.
Journal Information
- Title
- “Clinical factors associated with congenital cytomegalovirus infection: A cohort study of pregnant women and newborns”
- DOI
- 10.1093/cid/ciz1156
- Authors
- Akiko Uchida, Kenji Tanimura, Mayumi Morizane, Kazumichi Fujioka, Ichiro Morioka, Masanobu Oohashi, Toshio Minematsu, Hideto Yamada
- Journal
- Clinical Infectious Diseases